It will be breaking news to very few people that after the votes on 14th December 2021, the full set of nations in the UK now have “Covid Certification” or “vaccine passports” with the governments of England and Northern Ireland conclusively voting in favour to be a papers-please society, joining Scotland and Wales who have had them in place for several months.
Here in Northern Ireland, the Department of Health released their domestic “Covid Certification” app on the 1st November, The Executive voted in favour to make Covid Certification mandatory on 17th November, which were then introduced on the 29th November, becoming enforceable on 13th December, and finally, the assembly of MLAs voted in favour for it to remain in place on 14th December.
The rules now state, that to enter premises such as nightclubs, pubs and bars, restaurants and other entertainment venues, you must be able to prove full vaccination. If you can’t prove you’re fully vaccinated, you must show a negative test taken in the previous 48 hours, or proof of previous infection from 30-180 days prior to the day you attempt entry.
We have been doing our utmost to challenge the logic and rationale of the scheme, as well as requesting evidence that would show how the vaccine passports would be beneficial in terms of public health, and have published our findings in a series of articles. We have submitted Freedom of Information requests to The Executive, and the Department of Health, with no evidence being provided, claiming no such information was in their possession. Shortly after the vote by The Executive, the First Minister, Paul Givan, responded to emails to constituents advising no evidence had been presented, as well as no impact assessments being completed. Based on this, it has been difficult to understand on what grounds four of the five parties in The Executive had opted to vote in favour of a domestic Covid certification scheme.
Since then, “evidence” has been published. On 26th November, the Department of health, quietly, published, a document to their website titled “Scientific Evidence for COVID Certification”. It would appear that at this point, and during the following couple of weeks, that it wasn’t widely shared with either The Executive, The Assembly or the public, as demands for evidence continued and claims it didn’t exist continued right up to the debate ahead of the vote on 13th December.
During the debate, the TUV’s Jim Allister commented that members in The Executive, including the First Minister, had claimed evidence had still yet to be presented, to which the Health Minister, Robin Swann responded saying they had been offered the opportunity to view the evidence, but that only two other ministers took up the offer. We believe this document is the “evidence” that Robin Swann is referring to. Had the other ministers taken the opportunity to view and scrutinise this document, we’d have hoped that, like us, they would have been left with many questions regarding the quality of the evidence provided.
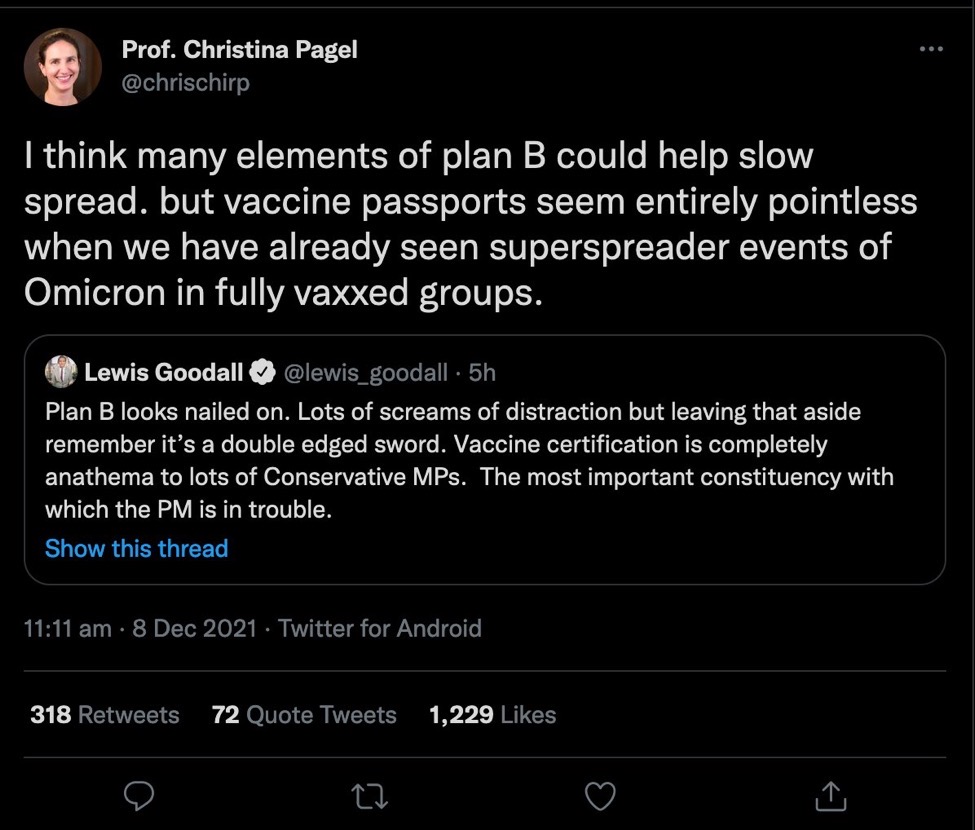
The Department of Health published a tweet on 14th December with a link to the evidence giving greater opportunity for public scrutiny:
You can follow the link to the tweet to view the responses which gives an indication of how members of the public view this evidence:
The “Scientific evidence for COVID certification” is a very short document, one and half A4 pages and references four supporting studies. Let’s break it down:
“SAGE noted in April 2021 that, in relation to COVID-19:
“There are three main ways in which baseline measures can reduce transmission (from most to least effective)”:
1. Reducing the likelihood that people who are infectious mix with others.
2. For those potentially infectious people who are not isolated, reducing the likelihood that they enter higher risk settings or situations.
3. Decreasing the transmission risk from a potentially infectious person in any given environment.”
This is in reference to a document published by SAGE, “Considerations in implementing long-term ‘baseline’ NonPharmaceutical Interventions (NPIs)”, and the three bullet points in the DoH document are headings to sections within the SAGE document. Important to note this document was published back in April 2021, and therefore the information and references included are prior to when the Delta variant was supposed to have become the dominant variant in the UK. We’ll summarise each section further to see what SAGE had to say at the time.
- Reducing the likelihood that people who are infectious mix with others
The measures in the section that SAGE refer to are:
- Test, Trace and Isolate – symptomatic and asymptomatic testing, contact test and trace, and other surveillance.
- Self-isolation is critical – Symptomatic isolation primarily.
- Quarantine after international travel
So, no mention of Covid certification for this section.
- For those potentially infectious people who are not isolated, reducing the likelihood that they enter settings or situations.
In this section, SAGE does refer to certification:
“One approach to this is certification (based on negative testing, vaccination, or proof of prior infection) that there is a lower probability that an individual is infectious, or that an individual will suffer severe symptoms if the virus is transmitted to them. This can in some cases be achieved via certification, though there are a number of practical and ethical issues to be considered, including whether any form of certification is equally accessible across the population and whether the certification is reliable.”
To support this proposal, SAGE references minutes from their meetings, SAGE 72, and SAGE 79:
This meeting was held in December 2020, right at the beginning of the Covid vaccination roll-out and therefore too early to assess the effectiveness of a mass vaccination programme. They did include some interesting points in terms of the vaccines:
“4. Whilst emerging data show that vaccines can offer good protection against disease, the degree of protection conferred against infection remains unknown. People who are vaccinated may still be able to become infected and to infect other people, though vaccination may reduce the risk. The impact of vaccination on the potential infectiousness of vaccinated people if they were to become infected is also currently unknown.”
Point 4 shows that at the time of the meeting, there is still a great deal of uncertainty with regards to transmission prevention with the vaccines, so this couldn’t be used by DoH as supporting evidence to offer entry to premises to those who are fully vaccinated and justify only testing those who are not.
“6. Different types of certificates (to show an individual is virus-free, has natural immunity or has been vaccinated) could lead to different behavioural responses. Pilot studies should be conducted to consider this, alongside ethical concerns, before the introduction of certification.”
Point 6 highlights that thoughts about the effectiveness of certification is in the early stages, and again this couldn’t have been used by the DoH as part of their evidence base.
This meeting was held in February 2021, which was the early months of the vaccine roll-out before it been offered to the whole population. Interesting points:
“3. Immunity certification could be used in addition to other measures to control transmission and/or to enable the relaxation of certain measures, but it is an imperfect tool and a risk-based approach should be adopted. The prevalence of infection in the community will have an important impact on the level of risk and effectiveness of certification (it may be very effective when prevalence is low, but less effective at high prevalence). Operational, behavioural and ethical issues all need to be considered for specific use cases. Pilot studies and randomised trials are recommended.”
As SAGE suggest pilot studies and trials are recommended, this indicates that at the time of this meeting, the effectiveness of such a scheme had not been established, and again is not evidence in favour of Covid Certificates or passports.
“29. Certification could be used in addition to other measures used to control transmission and/or to enable the relaxation of certain measures, but it is an imperfect tool and a risk-based approach should be adopted. The prevalence of infection in the community will have an important impact on the level of risk and effectiveness of certification (it may be very effective when prevalence is low, but less effective at high prevalence). The reliability of any immunity certificate will be reduced if virus variants with significant antigen escape are circulating.”
Omicron has dominated the headlines in recent weeks with initial analysis suggesting that the vaccines are less effective against it, including transmission prevention. Yet, this point suggests in a period of high prevalence, and with a variant with antigen escape in circulation, then an immunity certificate will have reduced effectiveness. Did the DoH miss this, or ignore it when gathering their evidence base for Covid certification, as we’re told that this is the situation we’re now in with Omicron? Or did they know this and choose to proceed with implementation despite this advice?
So, the SAGE document the DoH refers to is not evidence that Covid Certification will be of benefit to public health, it doesn’t claim to be, and regardless of that, it was published eight months ago during a completely different situation to now, and therefore is out of date.
We come back to the DoH paper, to the section which attempts to apply the logic for the introduction of Covid Certification, “Covid Certification will therefore have the following benefits”:
“It will reduce virus transmission, primarily by reducing the likelihood of infections (sic) individuals entering high risk settings”
Will it? And if so, by how much? People deemed fully vaccinated do not have to prove they’re not infected, only the unvaccinated are required to do that. This scheme is presently aimed at adults only, and this is the current vaccination rates in adults according to the DoH’s vaccination dashboard:
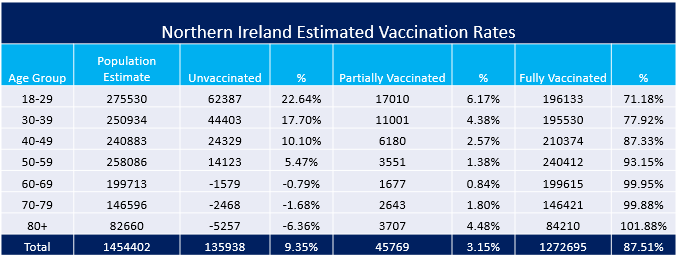
The population estimates are based on NISRA’s mid-year estimate for 2020, clearly they’re not completely accurate as in the older age groups more people have received at least one vaccine than the population estimate, but it does provide an indicative gauge of the population’s vaccination status. Based on this, 12.5% of adults are regarded as not fully vaccinated.
The UK Health Security Agency publish statistics on cases based on vaccination status, each report covering a four-week period. We’ve extracted the figures for the over 18’s and removed the “unlinked” cases, as they’re not applied to any of the vaccinated statuses, this is what their latest report looks like:
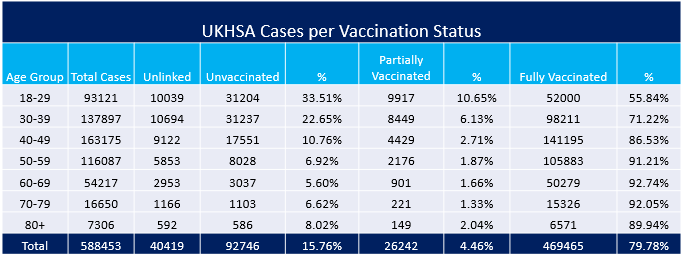
Using the UKHSA data, 80% of all adult cases are in the fully vaccinated, this is the population that do not have to prove that they are Covid free when entering hospitality premises.
Next point:
“Hence, it will reduce the risk of serious illness and death and in doing so alleviate current and future pressure on the healthcare system”
This point is following the assumption in the previous claim that Covid Certification will have a meaningful impact on reducing transmission, as we have already addressed, the real-world data does not support this claim as being fully vaccinated doesn’t prevent infection or transmission by a significant amount. At best, the new rules may filter out a small number of unvaccinated people who have tested positive using an LFT. Given that it is only the unvaccinated that have to prove they’re not infected suggests that it is them that are contributing greatly to the pressures in hospital and to the death statistics.
The Department of Health publish their “Vaccination status of deaths and hospitalisations” report every couple of weeks, with the latest covering the period 8th November to 5th December.
Hospitalisations:
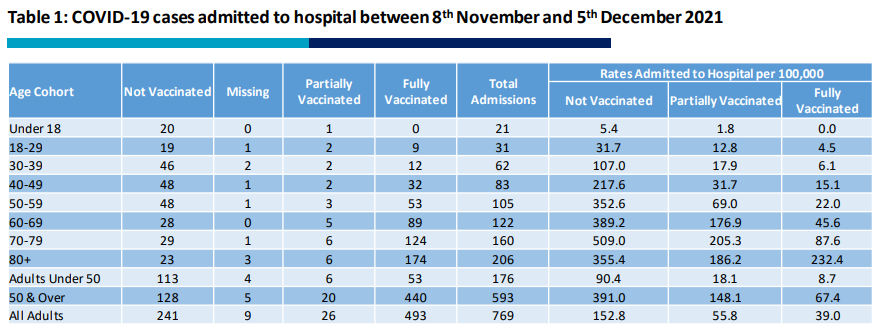
This table shows that the hospital admissions for those that aren’t fully vaccinated make up 267 of the total 769 admissions (34.7%) which does seem disproportionately high when compared to the size of the unvaccinated population. However, this information lacks context as it doesn’t provide enough detail, such as how long people are remaining in hospital.
The DoH daily dashboard data provides the admission and discharge dates, meaning we can calculate how long a patient remains in hospital with Covid. The extract for the same time-frame as the hospitalisations table above looks like this:
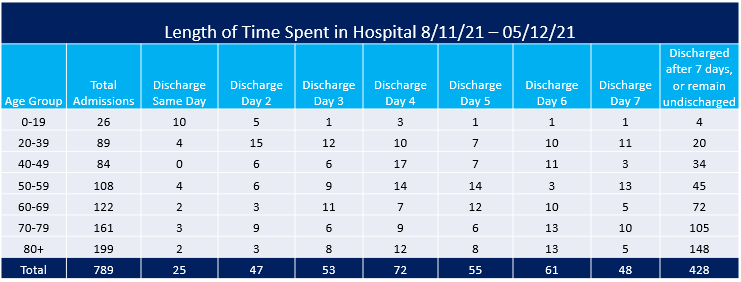
This shows a clearer picture of where the majority of resource is spent looking after patients with Covid:
- In the under 60’s the majority of the admissions are not fully vaccinated (191 vs 106) but the majority in these age groups are discharged within a week, 204 vs 103 who discharged after 7 days or more.
- In the over 60’s the majority of patients are discharged after 7 days or more, 325 vs 157 who are discharged within a week. According to the DoH report, only 97 patients over 60 are not fully vaccinated.
This shows the vast majority of hospital resource in terms of Covid is spent treating patients who are fully vaccinated. How will Covid Certification, which will impact younger age groups the most, alleviate a meaningful amount of pressure on the health service?
The DoH report also provides data on deaths:
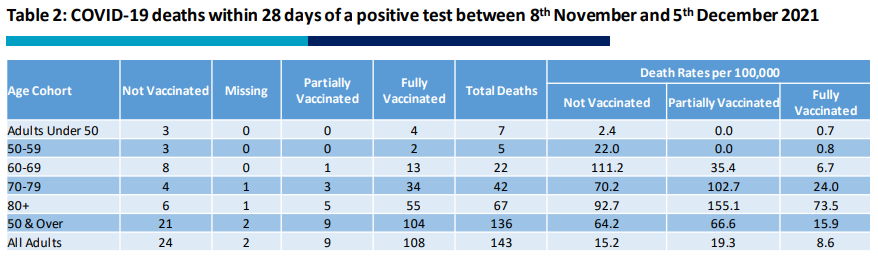
Adults under 50, who are more likely to be attending premises such as nightclubs and bars where there’ll be more people mixing, make up 7 out of the 143 deaths, with numbers as low as this, it is difficult to see how Covid Certification will have any meaningful reduction, if any reduction at all.
We come to the DoH’s final claim of main benefit:
“It will increase the likelihood that higher risk settings can continue to operate as an alternative to closure or more restrictive measures”
If this point is claiming the businesses affected by the new Covid Certificate rules are being protected by the new measures, then the immediate fall-out following the rules becoming enforceable is not proving the case.
Citizen Journos reported on 15th December 2021, “Vaccine Passports are destroying Northern Ireland hospitality” highlighting the waves of cancellations and major reductions in footfall that hospitality is experiencing.
The businesses, which we’re told Covid Certificates are put in place to protect, are coming under immense financial pressure as a result of these very “Certificates”, and at a time which should be their busiest & most profitable period of the year.”
This concludes the three claims made in the “scientific evidence” report, and it is very clear to see how unrealistic they are in the real world. So what evidence are they using to back these claims up? This bring us to the secondary benefit claims in the DoH paper.
The paper contains links to 4 studies and Twitter user @WrecklessGamer quite rightly highlights the problems with the “evidence” in the following thread:
“There is also likely to be a secondary benefit in relation to increased vaccine uptake
There is overwhelming evidence that vaccination reduces the risk of becoming infected with the virus and in particular that it reduces the risk of serious illness requiring hospitalisation.”
The DoH paper links this claim to the first paper listed in the references, “VEEP Vaccine Effectiveness Table” which was published on 7th October 2021. This is the first table in the document detailing the vaccines’ effectiveness against the Delta variant:
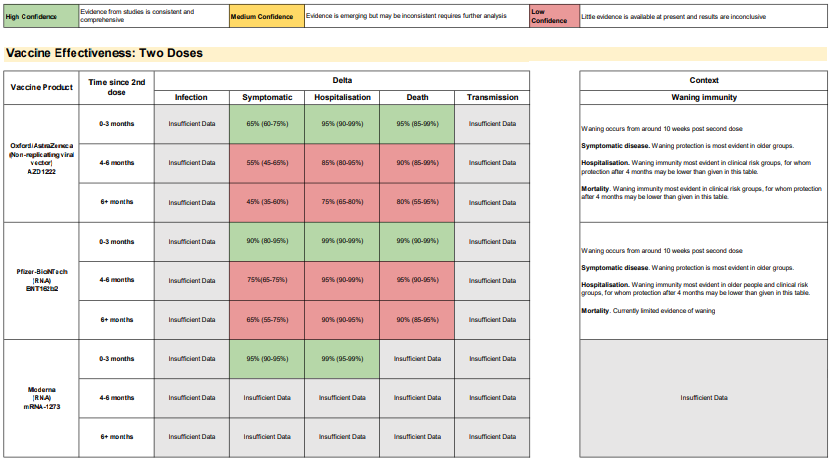
For all three vaccines, the table states “Insufficient Data” for both infection and transmission, so this can’t be used as the “overwhelming evidence” that vaccination reduces risk of being infected with the virus, as that data isn’t provided in this document even though the Delta variant had arrived approximately 5 months prior to this it being published. In addition to this, Omicron is the latest variant of concern, so there will be even less data for vaccine effectiveness.
The document also highlights that for Symptomatic, Hospitalisation and Death, only has high confidence in the first 3 months after vaccination, thereafter, the claims of effectiveness are assigned as low confidence. Covid certification based on vaccination status doesn’t specify the length of time since last vaccine, yet.
“In addition, there is recent evidence that in the event of a vaccinated individual becoming infected with the delta variant, they have a reduced likelihood of transmitting the virus to others”
This claim links to two studies in the references. Both are preprints and are not peer reviewed.
- Eyre DW et al, The impact of SARS-CoV-2 vaccination on 1 Alpha & Delta variant transmission. medRxiv preprint.
- de Gier, B et al. Vaccine effectiveness against SARS‐CoV‐2 transmission to household contacts during dominance of Delta variant (B.1.617.2), August‐September 2021, the Netherlands. medRxiv preprint doi:
Both studies claim that vaccination reduces transmission of the Delta variant, the dominant variant at the time of publishing, in October 2021. But as the UKHSA data shows, the fully vaccinated population are catching and spreading the virus at high rates, therefore the impact on reducing transmission can’t be very high in the real-world.
Regardless of the accuracy of the reports, which is questionable, they are preprints, and it states at the top of each report:
“This article is a preprint and has not been peer-reviewed [what does this mean?]. It reports new medical research that has yet to be evaluated and so should not be used to guide clinical practice.”
These articles should not be used as evidence to form public policy, and the question should be asked why the DoH have chosen to use these as their evidence base instead of peer-reviewed research – does the research that supports their claims not exist in that form?
The final referenced study is one we have come across before. In our previous article, First Minister Confirms No Evidence for Vaccine Passports, we discussed the study “The impact of mandatory COVID-19 certificates on vaccine uptake: Synthetic Control Modelling of Six Countries” as it had been provided by Northern Ireland MLA, Mike Nesbitt, to a constituent who had raised concerns about the impending Vaccine Passports.
The DoH scientific evidence report references the study to back up this claim:
“In addition, there is evidence that the use of mandatory COVID-19 certificates leads to an increase in vaccine uptake, which will make a further contribution to reducing infections and protecting against sever (sic) illness requiring hospital admission.”
This study is also a pre-print, and as we previously had proven, it contained out of date information. The study’s main aim was to show increased vaccination uptake when vaccine passports were implemented in the six countries – Denmark, Israel, Italy, France, Germany and Switzerland. However it had noted a secondary benefit in reducing transmission and included this graph:
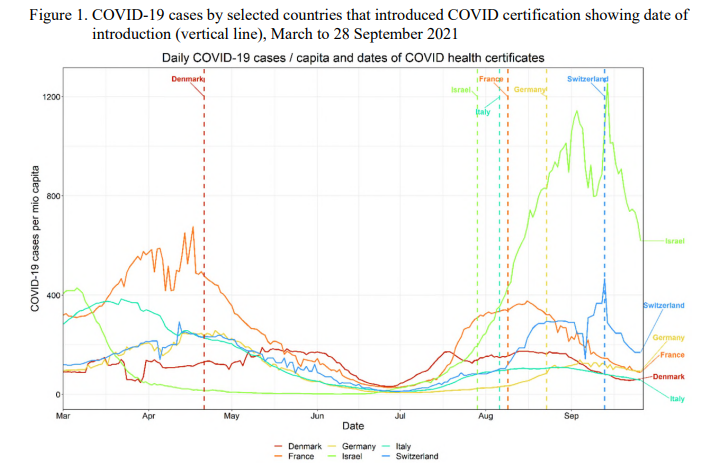
At the time the European countries seemed to show a reduction in transmission post implementation of the vaccine passports, while cases in Israel continued to rise over the following month before decreasing. As in our previous article, the following graph from Our World in Data, shows what happened to case rates in those countries after the cut-off date on the graph in the study, 28th September 2021:
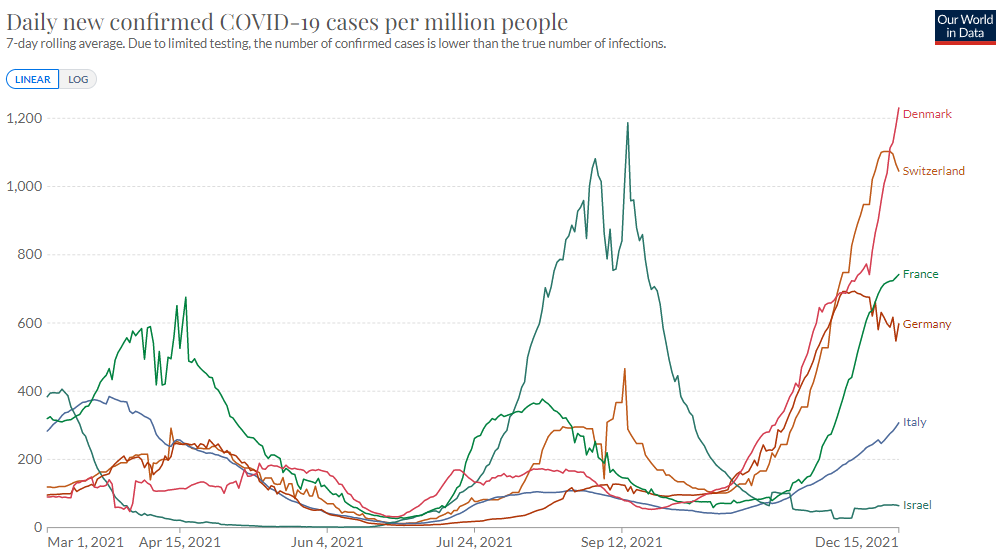
Extending the graph to the present day shows a completely different picture to the graph in the Oxford study. All the European countries showing increases in case numbers, with very high rates in Denmark, Switzerland, France and Germany. Strangely, Israel is again the outlier with case numbers remaining low, could this indicate a seasonal effect? The study surely wouldn’t have claimed the benefits of reduced transmission using this up to date information, and also goes against the claim in the DoH report that an increased vaccine uptake would reduce transmissions, yet they made the claim and used out of date information from an non-peer-reviewed study to support it.
The primary claim of the study is that mandatory Covid certification will have an impact by increasing vaccination uptake, but even that claim is questionable, which is highlighted in these studies in The Lancet and the BMC:
Behavioural responses to Covid-19 health certification: a rapid review – BMC
Using the evidence we have analysed above The Executive voted in favour of introducing Covid Certification six votes to four. Four parties in favour and one party against.
Followed by a vote in the Northern Ireland Assembly, which was 59 in favour, and 24 against, a conclusive victory.
The votes mean we now have mandatory, enforceable Vaccine Passports, based on “evidence” that is completely out of date, incorrect and supported by studies which are out of date, incorrect, and non-peer-reviewed preprints.
Combine the flimsy health “evidence” with the fact that no societal or economic impact assessments had been carried out prior to their introduction, we must conclude that this policy, which commenced development in April 2021, was being introduced no matter what.
Desperate to support the proposal following repeated questions (and FOI’s) from members of the public and occasionally a persistent MLA or two – This was all they could find.
It simply does not stack up.