
Chief medical officers of the UK approve and recommend universal Covid vaccination programme for 12 to 15 year-old children.
On the 14th September 2021, the Department of Health for Northern Ireland announced the Covid-19 vaccine will be offered to all 12 to 15 year olds following unanimous advice from the four UK Chief Medical Officers.
They decided to progress the rollout to this cohort in spite of the fact the Joint Committee on Vaccinations and Immunisation (JCVI) less than two weeks prior stated they could not support a universal programme of vaccinating healthy 12 to 15 year-old children at this time. The following is a segment from the JCVI’s statement published on the 3rd September 2021, which provides the basis for their advice:
The available evidence indicates that the individual health benefits from COVID-19 vaccination are small in those aged 12 to 15 years who do not have underlying health conditions which put them at risk of severe COVID-19. The potential risks from vaccination are also small, with reports of post-vaccination myocarditis being very rare, but potentially serious and still in the process of being described. Given the rarity of these events and the limited follow-up time of children and young people with post-vaccination myocarditis, substantial uncertainty remains regarding the health risks associated with these adverse events.
Overall, the committee is of the opinion that the benefits from vaccination are marginally greater than the potential known harms (tables 1 to 4) but acknowledges that there is considerable uncertainty regarding the magnitude of the potential harms. The margin of benefit, based primarily on a health perspective, is considered too small to support advice on a universal programme of vaccination of otherwise healthy 12 to 15-year-old children at this time. As longer-term data on potential adverse reactions accrue, greater certainty may allow for a reconsideration of the benefits and harms. Such data may not be available for several months.
JCVI statement on COVID-19 vaccination of children aged 12 to 15 years: 3 September 2021
The Chief Medical Officers of the UK took just ten days to provide an overrule to the JCVI advice, and have decided to proceed with the roll out to this age group, indicating they are less concerned regarding the potential harms identified in JCVI’s statement, including the condition, myocarditis.
Dr Michael McBride’s position regarding this decision is curious. Since the beginning of the school year there have been many reports of entire classes being sent home due to the covid contact-tracing policy in schools, which prompted Dr McBride to issue a letter to parents, pupils and schools on the 9th September 2021. The letter can be viewed in full here.
Here’s a few key highlights from Dr McBride’s letter:
“Having examined the evidence, I am confident that now is the right time to introduce a more targeted approach to the identification of close contacts of COVID cases in schools.”
”The English study found that over 98% of school close contacts did not develop COVID during the isolation period. Similarly the Scottish study found that 95% did not go on to develop COVID during the isolation period. Both included a period when Delta was emerging.”
“Public Health Agency (PHA) has analysed data on over 18,000 students from our own schools who were asked to isolate because they were close contacts in school and the findings are very similar to those from those in Scotland.”
“There is clear evidence of a very low rate of severe disease in children of primary and secondary school ages even if they do catch the disease.”
Dr McBride acknowledged the disruption caused by the previous contact tracing policy and that it needed to be adjusted to reduce the impact on schools. He then referred to studies which would suggest transmission amongst school children was low, as 95%+ of pupils identified as close contacts would not develop covid. Dr McBride also reassured schools and parents that children are at very low risk of suffering severe illness from Covid-19.
Yet, the weekend passes, and on the Monday, it is announced that this group is recommended for vaccination for a disease, which the Chief Medical Officer himself stated a few days earlier, is of negligible risk to them and of which they are not significant drivers of transmission.
The low risk to children claim that Dr McBride makes is backed up by the Department of Health’s own data they use to populate the Covid-19 daily dashboard.
NISRA published their population estimates for 2020, which states the age group 0-15 equated to 20.9% of the population in Northern Ireland, which is approximately 397,000 children in this group.
The Covid Dashboard doesn’t break the age groups down in the same way as the NISRA population report, but the age group 0-19 will provide a rough idea of the covid-19 impact on this age group.
Since March 2020, in the 19 years old and under age group:
- Hospital admissions – 217 out of 12,221 (1.78%)
- Hospital Inpatients at midnight (this represents the number of overnight stays patients remained in hospital) – 1016 out of 312,832 (0.33%)
- Covid Recorded Deaths – 2 out of 2478 (0.08%)
The above statistics are based overall 0 to 19 age group, indicating that the impact on the 12-15 age group will be less.
Using the estimated population (0–15 year-old) totals – the maximum risk is as follows:
- Hospital admissions – 217 out of 397,000 (max. 0.05%)
- Covid recorded deaths – 2 out of 397,000 (max 0.0005%)
One of the ‘Covid record deaths’ in the 0-19 year old category has previously been highlighted and the categorisation as a ‘covid death’ has been disputed. You can read more on that here.
A recent Freedom of Information request to the Department of Education (DoE), also supports Dr McBride’s view in his letter, that children are not major drivers of transmission.
The request sought to understand the level of absence from schools due to the contact-tracing policy and confirmed cases of Covid-19.
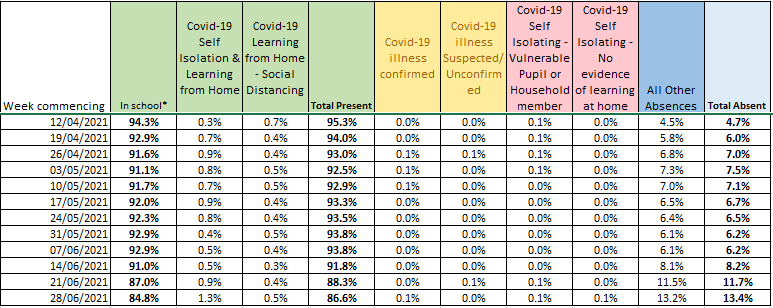
The data provided by the Department of Education confirms that in the 12-week period shown:
- The maximum volume of pupils absent due to covid-19 confirmed illness was 0.1%.
- Suspected Covid-19 recorded as 0.1%.
- The rest of the weeks were recorded as 0.0% which suggests that some rounding up and down was done in the populating of the data, but still confirm the actual impact to be very small.
- The combined Self Isolation and Social Distancing percentages, while are higher than confirmed or suspected illness, show that at most 1.8% were studying from home as a precaution. That said, the vast majority did not go on to develop Covid-19.
It is clear from the data that as an illness, the threat of Covid-19 to children, particularly healthy children, is negligible.
So, what benefits could there be that made the CMO’s take the decision that they should be vaccinated for this disease?
Covid: Children’s education ‘will benefit’ from jab move – BBC NI – 14/09/2021
“Offering jabs to children aged 12 to 15 will help avoid damage to their education and life chances, NI’s chief medical officer has said.”
In this BBC article, Dr McBride makes the case that vaccination will offer children the chance of a much less disrupted education, this is despite making changes the previous week to the contact tracing policy in schools, which should result in fewer pupils being sent home due to someone else receiving a positive test result.
Dr McBride’s decision suggests that the protection of children’s education is the prime benefit, rather than the benefits clinically.
On the 13th September 2021, the Department of Health and Social Care for England published their report – Impact on school absence from COVID-19 vaccination of healthy 12 to 15 year old children.
In this report they present scenario-based estimates of school absences due to Covid-19, with and without vaccination, for the period 18th October 2021 to 31st March 2022. The scenarios and data included allow a calculation of how much school absence they think will be saved on average per pupil.
For this calculation their ‘Main Scenario’ was used.
Key points for this estimate:
- There are approx. 2,240,000 million healthy 12 to 15 year-old children in England.
- There are approx. 100 days in school between 18/10/21 and 31/03/22, making a total combined 224,000,000 days all pupils will attend school.
- Main scenario: No vaccination – 320,000 total days absent due to Covid-19
- Main scenario: With vaccine – 220,000 total days absent due to Covid-19 (100,000 days reduction)
The 100,000 total days reduction with vaccination, equals 0.04% of the total 224,000,000 total combined days pupils attend school. Based on a 9am-3pm school day, taking account of breaks, equals 5 hours schooling per day. 0.04% of a 5 hour school day, equals around 8 seconds. 8 seconds multiplied by 100 school days for the period covered in the report, equals approx. 13 and a half minutes.
13 and a half minutes.
Following the roll-out of the vaccine to healthy school children in the 12-15 age bracket, they expect it’ll save on average per pupil 13.5 minutes of absence due to Covid-19 over a six-month period.
What the report hasn’t considered is – How long does it take to administer the vaccines? How long does each pupil have to sit and rest after a vaccine being administered? What if a child has an adverse reaction, even if mild, and takes time off school, how many shares of 13.5 minutes will that absorb until all the benefit is wiped out?
What if the adverse reaction a child experiences is severe? Like myocarditis, which the JCVI acknowledged in their statement as rare but potentially serious?
Consideration of myocarditis as an adverse reaction to Covid vaccines is growing, as evidenced by the JCVI including it as part of their assessment to not recommend a universal administration programme to children.
The British Heart Foundation define myocarditis as – “Myocarditis is inflammation of the myocardium – the heart muscle. Most people with myocarditis recover without any complications but in rare cases when inflammation is severe, there can be damage to the heart.”
More information on post-vaccination myocarditis can be found in this not yet peer-reviewed article. A group of doctors in the U.S have submitted this article to the medRvix site based on data in the Vaccine Adverse Event Reporting System (VAERS). The article claims that, based on VAERS data, following the second dose of an mRNA vaccine, 162.2 per million males aged 12-15 suffered myocarditis post-vaccination, and females in the same age group were 13 per million.
There has been confusion amongst the UK population for some time with regards to contradicting messages from governments in relation the COVID-19 policies and decisions but this decision must be one of the most confusing.
The JCVI have highlighted adverse reactions such a myocarditis as rare but were not prepared to approve the use of covid vaccines for 12 – 15 year olds at this time.
Dr McBride states that ‘There is clear evidence of a very low rate of severe disease in children of primary and secondary school ages even if they do catch the disease’.
The government’s calculation of benefit relies solely on school attendance figures rather than clinical benefit and even that benefit is miniscule. Yet the covid-19 vaccines have been approved for use in 12-15 year-olds. It is difficult to see how this conclusion was reached and these mixed messages will only serve to confuse parents who only want what is best for their children.